
This is not a new blog piece, but a sincere thank you to all for the support and positive, thoughtful comments about “In My Hands”, which was released by the Hachette Book Group on May 22. I deeply appreciate all … Continue reading
This is not a new blog piece, but a sincere thank you to all for the support and positive, thoughtful comments about “In My Hands”, which was released by the Hachette Book Group on May 22. I deeply appreciate all … Continue reading

At the risk of sounding superstitious and nonscientific, I have observed in oncology practice we sometimes have “streaks.” Some of these are positive winning streaks where our patients are responding well to therapy, their operations are successful and they recover … Continue reading
When I was a medical student, it was recommended we read “On Death and Dying” by Elizabeth Kubler-Ross. This book is considered foundational and established five stages people facing death go through: denial, anger, bargaining, depression, and acceptance. I don’t recall specifically which one of my professors recommended this book, but I did read it and found it useful in understanding how people respond to the grim news they have a disease that may or will lead to their demise.
Dr. Kubler-Ross’s book was instructional, but years of performing major surgical procedures attempting to prevent patients’ deaths from malignant disease have taught me that not everyone goes through all five stages. I have one notable and memorable patient who started in the first stage, and has remained in the second stage (with occasional visits back to the first stage) for over 25 years now. And she hasn’t died despite having stage 4 cancer, so it’s working well for her.
The patient I am thinking of was a lady in her mid-50’s when she was referred to me by a gastroenterologist. She had seen the gastroenterologist because she was having bleeding with bowel movements over a three-month period. The gastroenterologist performed a colonoscopy and visualized and biopsied a tumor in her sigmoid colon. The biopsy demonstrated a malignant colon cancer, so he sent her to me for surgical care. He did not provide any warning about her mindset.
At her initial consultation visit with me, I walked into the room and introduced myself to her and her husband. The look on her face and the energy in the room was pure anger. Her husband sat three or four feet away from her, not making eye contact with her at any time. My first inquiry was to ask how it was she came to be diagnosed with colon cancer.
I was startled by the vehemence of her response. “I DO NOT HAVE CANCER!” Confused, I looked at the sheet of color pictures taken during her colonoscopy demonstrating a tumor in her sigmoid colon. I glanced again at the pathology report indicating a colon adenocarcinoma. I confirmed her name and date of birth was on both of these pieces of information. I looked up and my gaze met hers, and I asked her to explain.
The patient informed me she had no family history of cancer, she lived a healthy lifestyle, she did not smoke cigarettes, she did not drink alcohol, she was not overweight, she exercised regularly, and she had no other medical problems. Therefore, it was impossible for her to have cancer. I was mildly abashed. I had not previously encountered denial of this vigor and intensity. I mentioned that the reports from her referring physician suggested she did have a malignant tumor in her colon. She vigorously shook her head from side to side and said, “No! The doctor is wrong.”
I excused myself from the room and went out to look at the CT images we had obtained. They showed a definite mass in the sigmoid colon, but no evidence of any enlarged or abnormal lymph nodes or metastatic tumors in the liver or lungs. I returned to the room, feeling stymied about how best to approach this patient. At this point, for the first time, her husband looked up at his wife and made a simple statement, “You know dear, you may not believe it, but you do have colon cancer. “
The patient shot him a withering look and he sat frozen in position, with the immediate development of a grey pallor to his skin. I instantly thought of the story from Greek mythology of Medusa; a single look at her face and hair made of wriggling snakes would turn any mortal into stone. The look from the patient was so fierce that I involuntary pushed my wheeled stool two feet back away from her. I glanced over at the patient’s husband, and after seeing he was quietly respiring and occasionally blinking his eyes, I turned back to his furious wife. The conversation that ensued was unique in my experience. She was undeterred in her belief the cancer diagnosis was incorrect. She went on to explain to me over the next twenty minutes that she would prove to me she did not have colon cancer. She stated she had been doing “quite a bit of research” and had found some special high fiber natural diets that would cleanse her system of any malignant cells. I informed her that my recommendation was that she allow me to perform a sigmoid colon resection to remove her biopsy-proven colon cancer. This pronouncement was met with a sneer and a denigrating remark, “You doctors think you know everything and just want to cut people up.”
Okey dokey. I had made a standard of care recommendation for surgical treatment but this lady denied the presence of any malignant disease. She was so certain her physician was incorrect in his diagnosis that she promised to return in three months after eating her special diet to allow me to repeat her endoscopy. I had no choice but to agree. I can recommend a surgical procedure or a multidisciplinary treatment regimen, but I cannot and will not force anyone to comply.
Three months later, as agreed, the patient and her docile husband appeared in my clinic. My nurse instructed her how to administer two enemas to cleanse her lower colon. She completed this task, and I then inserted a flexible sigmoidoscope into her rectum and directed it upstream into her colon. There, 25 cm up into her colon was a slightly larger, but still non-obstructing colonic tumor. I took photographs through the scope and biopsied the tumor. I informed the patient that I still saw the tumor, and even had her and her husband look through the scope. After withdrawing the scope, I temporarily departed and the patient got dressed. I returned to the room to find the patient and her husband, the latter speechless throughout the entire interaction, seated in two chairs. Rather than being contrite, she smugly said, “Let’s just see what those biopsies show, shall we?” I politely agreed and made an arrangement to call her the following week when the biopsy results returned.
The biopsy confirmed colonic adenocarcinoma. I dutifully called the patient and informed her that she had a sigmoid colon cancer, now proven by two sets of biopsies. The phone line was silent for almost ten seconds, and then she cut loose with a string of curses. She explained to me (unnecessarily) that she was very angry and she just did not understand how this was possible. I allowed her to vent for several minutes and once she had calmed down, I asked if she would permit me to schedule an operation to remove her colon cancer. With an exasperated tone, she agreed to allow me to proceed.
The next week I performed a routine sigmoid colectomy that went well. The patient recovered from the operation uneventfully and was discharged on her fifth post-operative day. When she saw me the following week in clinic for her first post-operative visit, I explained the pathology showed a cancer that had invaded into only the superficial muscle layers of the colon and, fortunately, there was no spread of the cancer into any of the nineteen lymph nodes we had removed during the operation. She had what we designate as stage II disease, and at the time there were no clinical studies indicating any clear benefit for giving chemotherapy in this situation. She asked for a copy of her pathology report, which I provided. She read the description line by line, asking frequent questions about specific terminology and meaning. At the end of a ten minute interrogation about the pathology report, she looked at me suspiciously and asked, “So you’re sure this is cancer?”
Yes, I was sure. I informed the patient and her obsequious husband that I recommended a follow up visit in six months with a cancer blood test and a year following surgery we should perform a repeat colonoscopy. She begrudgingly agreed.
At her six-month visit, her blood tests was normal. At her one-year visit, the colon cancer blood test, called a serum CEA, was elevated to almost ten times normal. Her colonoscopy revealed no colon tumors or polyps. I explained to the patient and her husband the abnormal serum tumor marker was worrisome, and after a twenty-minute negotiation, she agreed to a CT scan of the chest, abdomen, and pelvis.
The CT scan was obtained, and a single liver metastasis near the surface of the right lobe of her liver was identified. I walked into the examination room armed with the CT images and showed them to the patient and her husband. Once again an aura of fury permeated the room. The patient repeatedly stated it was not possible for her to have recurrence of her cancer. She reiterated she was doing everything right and could not understand how cancer could have reappeared. At one point she looked at me and declared, “You took all of the cancer out of my colon. It is impossible for it to now be in my liver.”
I calmly explained how a malignant colon tumor can spread to lymph nodes or can invade into microscopic blood vessels in the wall of the colon and release cells that then implant in another organ. I indicated the liver is a common place for colon cancer to spread and eventually grow into a tumor we can detect. I also informed her it was possible to remove this solitary tumor nodule, and then consider a course of chemotherapy in an attempt to eradicate any other microscopic cancer cells possibly present in her body. Finally, I mentioned surgical removal of the liver tumor followed by chemotherapy was not guaranteed to prevent the cancer from recurring in the future.
She sat in her chair fuming. You think he would have learned, but her husband stepped in it again. “Dear, you need to let Dr. Curley take care of this for you.”
Medusa returned. A medical student and a surgical resident had accompanied me into the examination room for my conversation with the patient and her husband. When the patient whirled with a face of rage directed at her husband, a quiet gasp escaped from the medical student standing behind me. I interceded before the patient could say anything and spent the next twenty minutes explaining in detail how the operation could potentially help her control and beat this cancer. I based my opinion on published data and reiterated we could potentially provide an effective treatment by removing this tumor. After continuing to fire occasional sidelong warning glances at her husband, she finally agreed to an operation. When we walked out of the room, the medical student and resident looked at me and the student said, “Wow! That look could have melted metal.”
Yeah, it was that searing.
The diagnosis of recurrent cancer was crimping the patient’s style, so I waited three weeks to perform her liver resection while she took care of other business and matters at home. I was able to perform a segmental liver resection removing only ten percent of her liver. Once again, she recovered uneventfully. The intra-operative ultrasound failed to reveal any additional liver tumors and my survey of the entire abdominal cavity showed no evidence of spread of disease at any other site. I presented the patient’s case at a multidisciplinary tumor board the following week and a plan for six months of adjuvant chemotherapy was recommended. It required over two hours of conversation and question-answering from me and one of my medical oncology colleagues, but the patient grudgingly agreed to receive the treatments. But only after I reconfirmed numerous times the tumor in her liver was actually metastatic malignant colon cancer.
I never witnessed this patient enter the bargaining, depression, or acceptance stages following her diagnosis of her stage 4 cancer. She was rooted in denial and anger. Who knows if this had any impact on her outcome, but I saw her back recently for a 25-year cancer-free follow up visit. The patient and her husband are older and moving much more slowly compared to when I first met them. Before I walked into the exam room, the patient’s husband quietly pulled me aside and informed me his wife had recently been diagnosed with Alzheimer’s disease. He remarked they would not be returning to see me for follow up visits, and he expressed his heartfelt appreciation for my care over the years. When I walked into the examination room and greeted my patient, I was met with the usual steely stare and expression of grim determination I was expecting. When I informed her she had no evidence of recurrent or new cancer, she merely nodded and said, “Of course I don’t have cancer.” I have never seen this patient smile. But I’ve been seeing her for over 25 years. I’m a happy man who likes a good joke and a laugh, but it’s not for everyone. As cancer clinicians, we see patients go through all five stages of emotions after a diagnosis of cancer. It is incumbent on us to recognize the stage, respond to the patients’ and their family’s questions and concerns, and help them move on with their life or prepare for a looming death.
Because we don’t know exactly how much life we have left, we might as well live the hell out of it.
I completed medical school more than 30 years ago. Medical education, like most aspects of life, has changed drastically in the past several decades with the advent of the Internet and electronic education programs and modules. I come from the pre-cellular telephone and personal computer era when dinosaurs like me carried loads of textbooks and sat dutifully through hours of classroom lectures taking copious notes. Frighteningly, I even recall college chemistry and physics classes where we were required to use a slide rule for mathematical calculations. Oh, the humanity!
At the time I was a medical student, most medical school curricula required you to spend your first two years in lectures and in laboratories learning anatomy, normal body functions, biochemistry, disease pathophysiology, pharmacology, diagnostic studies, and treatment options. All of us were excited and nervous in the summer of our third year because we were beginning our clinical rotations. The third year was comprised of three months of internal medicine, three months of surgery, and two months each of pediatrics, obstetrics/gynecology, and psychiatry. The fourth year of medical school had few required rotations and provided an opportunity to take electives specific or helpful in whichever career field a student had chosen. I enjoyed all of my third year rotations, despite realizing by fall of my third year that surgery was the career path making the most sense for me.
In the spring of my third year of medical school, I did a four-week rotation on a busy obstetrics service. It was great fun because the obstetrics faculty and residents allowed us to assist during normal deliveries, and then actually allowed students to deliver a few babies. The experience was certain to cause some tachycardia in the medical students, but after delivering the baby, clamping and cutting the umbilical cord, and handing the child to the mother, a sense of great accomplishment was assured. It was exhilarating and satisfying. I was glad I had played lots of sports like baseball, basketball, and football growing up; you need a sure set of hands as those new babies are slippery.
Over three decades later, I had not thought about delivering babies or anything to do with obstetrics. I am a surgical oncologist. The malignant or benign tumors I remove are a source of pain, angst, aggravation, and fear for my patients. After providing care for thousands of patients over the course of my career it is rare to encounter something that startles me. But I can still be surprised and I enjoy a good practical joke, even when played on me.
Several years ago a young woman not yet 30 years old was referred to me with a very large liver tumor. The patient had seen her local physician and reported she felt bloated and unable to eat a normal size meal. The referring physician examined her and was astonished to palpate a large abdominal mass. When I first walked in to the examination room to meet her and her husband, when she stood I wondered if she was pregnant. She had an obviously protuberant belly and I had not yet seen her magnetic resonance imaging (MRI) scans.
We spoke for ten or fifteen minutes and then I performed an abdominal examination. With her lying supine on the examination room table, it was possible to palpate a mass originating in her upper abdomen and extending well below her umbilicus. The mass was not tender but was firm. After completing the evaluation, I walked out and loaded the disk with her MRI scans onto my computer workstation. When I opened the abdominal images, I let out a low whistle. Quickly, every physician, resident, nurse, and student in clinic was clustered around the computer screen. A couple of representative images explaining their interest and excitement are seen in the two images below.

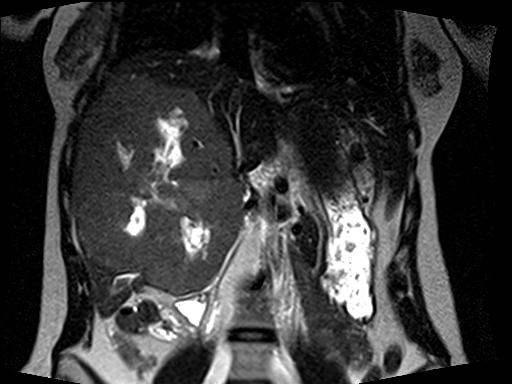
Almost the entire right lobe and the medial segment of the left lobe of her liver was occupied by an enormous tumor. There were areas of necrosis, or dead tissue, and other regions demonstrating recent hemorrhage, or bleeding into this tumor. The characteristics and MRI appearance were all consistent with a benign type of liver tumor called a giant cavernous hemangioma. The term giant was an understatement in this young lady. Hemangiomas are abnormal, but not malignant, spongy collections of blood vessels which can occur in many solid organs in the body. A familiar type of hemangioma is one arising in the skin (which is a large solid organ), known by the common vernacular name as a port wine stain.
This tumor was massive and clearly causing symptoms, so even though benign, I recommended surgical removal. I knew the operation would be a hepatobiliary surgery tour de force because the right and middle hepatic veins were compressed and the tumor abutted and bowed the main, left, and right portal veins.
Liver surgeons use a variety of specialized pieces of equipment to dissect through the liver and expose blood vessels and bile ducts that can be clipped, tied, or stapled to prevent bleeding or bile leakage. I was forced to make a larger abdominal wall incision than usual in this young woman once I recognized it would be necessary simply to remove the impressive tumor. The resident and I were able to mobilize the right side of the liver and take down its attachments to the tissue behind the liver and to the diaphragm. We used a special dissecting instrument with a rapidly vibrating tip to push aside the soft liver tissue while leaving blood vessels and bile ducts intact. The visualized vessels and ducts were then ligated, clipped, or if tiny, cauterized. We slowly and meticulously dissected through the liver and began the tedious process of dissecting the tumor free from the main and left portal veins, hepatic artery branches, and bile duct. We had to maintain normal blood supply to the remaining left liver and intact bile ducts to drain bile from the liver into the intestine. The numerous blood vessel branches running into the tumor were clipped or tied and divided. Once we had preserved the left sided blood vessels and bile ducts, I was able to staple and divide the blood vessels and the bile duct to the tumor-bearing right liver. We continued the careful dissection through the liver until we identified both the middle and right hepatic veins, and again it was possible to staple and divide these vessels. In a moment reminding me of some of the caesarean sections I had witnessed as a medical student, the resident and I gently wrestled the tumor mass out of the abdominal cavity, but, unlike the gentle swaddling of a newborn infant into a warm blanket, we indecorously plopped it into a very large basin we requested just for this purpose.
Returning our attention to the patient and the remaining portion of the left liver, we confirmed there was no bleeding or bile leak from the cut edge of the liver. Our blood loss for the operation was minimal. We checked the blood flow into and out of the liver using color flow ultrasonography. The liver was re-suspended to the diaphragm and the abdominal wall at the falciform ligament with a couple of sutures, and a drain was placed along the liver edge into the large empty space now present in the upper abdomen once occupied by a relatively gargantuan tumor. The patient recovered rapidly and without problems after her operation. She was young and in excellent health so she was walking the day after surgery and quickly developed a ravenous appetite. Nothing like having a large tumor compressing your stomach and intestine removed to improve your interest in food again. The patient was discharged from the hospital four days after the operation. Her drain tube was removed prior to discharge, and at her first post-operative visit she was recovering well and doing her best to ingest enough protein to permit liver regeneration. She succeeded well, and now has a large hypertrophied left lateral liver occupying her upper abdomen (see the representative image below).

On final pathology the patient did have a giant cavernous hemangioma, but the pathologist noted a few areas were worrisome for possible deterioration into a sarcoma-like situation. Her pathology slides were sent to multiple institutions and nobody was convinced she had an actual malignant tumor, but enough concern was raised I decided to follow her routinely for a few years to be certain no new tumors developed in the liver or at other sites. I saw her at six-month intervals with repeat MRI scans which confirmed there was no evidence of recurrent tumor. After about three years, I told her I was comfortable seeing her back on an annual basis. We did an annual visit and scans and blood tests were again completely normal. I had a social chat with the patient and her husband and learned she was involved in several new hobbies and activities. We ended the conversation with a pleasant goodbye and made plans for a visit a year later.
Seven months later I received an email from the patient requesting an urgent follow up appointment. Immediately alarmed and worried, I called my clinic staff to contact her for an appointment a few days later. When she arrived, I entered the examination room and was met by a somber-faced patient and her husband. She looked well but told me she was there to inform me of a new tumor. I asked if she was having symptoms to suggest the tumor had regrown. She solemnly shook her head no. I inquired if she had a disk with MRI scans for me to see. Another shake of the head no, and then she said, “All I have is this.” She handed me a black and white ultrasound image.
I’ve been a surgical oncologist for a long time, but thankfully my physical and mental facilities have not slowed yet. I studied the image for a few seconds, and by the time I looked up both my patient and her husband were grinning widely, and then openly laughing. She gleefully exclaimed, “I got you, didn’t I?”
Yes, yes you did. The ultrasound image revealed a normal human fetus of fourteen weeks gestation. I’ve performed thousands of ultrasounds of the liver, pancreas, and other upper abdominal organs or structures, but even though I’m not an obstetrician, I was quickly able to recognize the image of a human fetus. After the laughter and general hilarity waned and I congratulated them for playing the scene (and me) perfectly, we had an excited discussion about the elation and tribulations of parenthood. I shared stories from the time when my own children were small. I was thrilled for this young couple and this was not a conversation I had previously experienced in my practice. We agreed we would push the date of her next MRI scan to slightly longer than the originally planned one-year visit to allow her to complete her pregnancy.
A few weeks ago I noticed the patient’s name on my clinic schedule. I opened her MRI images and saw her enlarged left liver and no evidence of tumor recurrence. The scan also included the pelvic region and I noted a normal, non-pregnant uterus. I knocked once on the door, entered the room, and was immediately introduced to her new son. I have delivered lots of tumors out of patients’ bodies over the course of my career, but this remarkable, alert, healthy delivery brought a smile of pure happiness to my face. Removing malignant tumors from patients is rewarding, challenging, and often provides the best chance for a patient to be cured of this dread disease. I derive great satisfaction from the blessing of helping cancer patients, but holding this infant was a feeling of deep gratification surpassed only by the times years ago when I was embracing my own children. I hugged my patient and her husband and quickly reported everything was fine with her blood tests and scans. We spent the next twenty minutes watching her newborn son while talking about the fatigue, sleeplessness, and fulfillment associated with an infant. She was tired, but triumphant. As she left, she waved goodbye and stated, “I could have never had him with that huge tumor inside me.”
It certainly would have been crowded in her abdominal cavity with both a giant liver tumor and a full term infant present. I’m glad the removal of the liver tumor went so well and she is fully living and enjoying life. And more importantly, she has now created new life and will experience all of the joy, pleasure, fatigue, frustration, and induction of gray hair associated with this phenomenon.

Recently, as I do numerous times every week, I knocked on a clinic exam room door, opened it, and walked in. The tall cowboy put his hands on his knees and slowly unfolded himself from the chair. He gave me … Continue reading

I slowly opened the door to a patient room on the surgical floor and quietly walked up to my patient’s bedside one day a few weeks ago. It was late afternoon on the day I had operated on this lady. … Continue reading

Sensory abilities and acuity vary drastically from person to person. Some people have partial or complete loss of one or more of their five primary senses. They must adapt to the world around them using their remaining neurosensory capabilities. The … Continue reading

I took the long walk today. The long walk from the operating room to the frozen section pathology suite to the physician’s locker room (to grab my white coat) to a consultation room in the surgical waiting area. The family … Continue reading
