
This is not a new blog piece, but a sincere thank you to all for the support and positive, thoughtful comments about “In My Hands”, which was released by the Hachette Book Group on May 22. I deeply appreciate all … Continue reading
This is not a new blog piece, but a sincere thank you to all for the support and positive, thoughtful comments about “In My Hands”, which was released by the Hachette Book Group on May 22. I deeply appreciate all … Continue reading

At the risk of sounding superstitious and nonscientific, I have observed in oncology practice we sometimes have “streaks.” Some of these are positive winning streaks where our patients are responding well to therapy, their operations are successful and they recover … Continue reading
I completed medical school more than 30 years ago. Medical education, like most aspects of life, has changed drastically in the past several decades with the advent of the Internet and electronic education programs and modules. I come from the pre-cellular telephone and personal computer era when dinosaurs like me carried loads of textbooks and sat dutifully through hours of classroom lectures taking copious notes. Frighteningly, I even recall college chemistry and physics classes where we were required to use a slide rule for mathematical calculations. Oh, the humanity!
At the time I was a medical student, most medical school curricula required you to spend your first two years in lectures and in laboratories learning anatomy, normal body functions, biochemistry, disease pathophysiology, pharmacology, diagnostic studies, and treatment options. All of us were excited and nervous in the summer of our third year because we were beginning our clinical rotations. The third year was comprised of three months of internal medicine, three months of surgery, and two months each of pediatrics, obstetrics/gynecology, and psychiatry. The fourth year of medical school had few required rotations and provided an opportunity to take electives specific or helpful in whichever career field a student had chosen. I enjoyed all of my third year rotations, despite realizing by fall of my third year that surgery was the career path making the most sense for me.
In the spring of my third year of medical school, I did a four-week rotation on a busy obstetrics service. It was great fun because the obstetrics faculty and residents allowed us to assist during normal deliveries, and then actually allowed students to deliver a few babies. The experience was certain to cause some tachycardia in the medical students, but after delivering the baby, clamping and cutting the umbilical cord, and handing the child to the mother, a sense of great accomplishment was assured. It was exhilarating and satisfying. I was glad I had played lots of sports like baseball, basketball, and football growing up; you need a sure set of hands as those new babies are slippery.
Over three decades later, I had not thought about delivering babies or anything to do with obstetrics. I am a surgical oncologist. The malignant or benign tumors I remove are a source of pain, angst, aggravation, and fear for my patients. After providing care for thousands of patients over the course of my career it is rare to encounter something that startles me. But I can still be surprised and I enjoy a good practical joke, even when played on me.
Several years ago a young woman not yet 30 years old was referred to me with a very large liver tumor. The patient had seen her local physician and reported she felt bloated and unable to eat a normal size meal. The referring physician examined her and was astonished to palpate a large abdominal mass. When I first walked in to the examination room to meet her and her husband, when she stood I wondered if she was pregnant. She had an obviously protuberant belly and I had not yet seen her magnetic resonance imaging (MRI) scans.
We spoke for ten or fifteen minutes and then I performed an abdominal examination. With her lying supine on the examination room table, it was possible to palpate a mass originating in her upper abdomen and extending well below her umbilicus. The mass was not tender but was firm. After completing the evaluation, I walked out and loaded the disk with her MRI scans onto my computer workstation. When I opened the abdominal images, I let out a low whistle. Quickly, every physician, resident, nurse, and student in clinic was clustered around the computer screen. A couple of representative images explaining their interest and excitement are seen in the two images below.

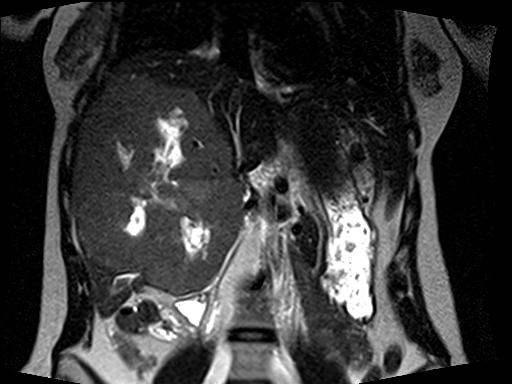
Almost the entire right lobe and the medial segment of the left lobe of her liver was occupied by an enormous tumor. There were areas of necrosis, or dead tissue, and other regions demonstrating recent hemorrhage, or bleeding into this tumor. The characteristics and MRI appearance were all consistent with a benign type of liver tumor called a giant cavernous hemangioma. The term giant was an understatement in this young lady. Hemangiomas are abnormal, but not malignant, spongy collections of blood vessels which can occur in many solid organs in the body. A familiar type of hemangioma is one arising in the skin (which is a large solid organ), known by the common vernacular name as a port wine stain.
This tumor was massive and clearly causing symptoms, so even though benign, I recommended surgical removal. I knew the operation would be a hepatobiliary surgery tour de force because the right and middle hepatic veins were compressed and the tumor abutted and bowed the main, left, and right portal veins.
Liver surgeons use a variety of specialized pieces of equipment to dissect through the liver and expose blood vessels and bile ducts that can be clipped, tied, or stapled to prevent bleeding or bile leakage. I was forced to make a larger abdominal wall incision than usual in this young woman once I recognized it would be necessary simply to remove the impressive tumor. The resident and I were able to mobilize the right side of the liver and take down its attachments to the tissue behind the liver and to the diaphragm. We used a special dissecting instrument with a rapidly vibrating tip to push aside the soft liver tissue while leaving blood vessels and bile ducts intact. The visualized vessels and ducts were then ligated, clipped, or if tiny, cauterized. We slowly and meticulously dissected through the liver and began the tedious process of dissecting the tumor free from the main and left portal veins, hepatic artery branches, and bile duct. We had to maintain normal blood supply to the remaining left liver and intact bile ducts to drain bile from the liver into the intestine. The numerous blood vessel branches running into the tumor were clipped or tied and divided. Once we had preserved the left sided blood vessels and bile ducts, I was able to staple and divide the blood vessels and the bile duct to the tumor-bearing right liver. We continued the careful dissection through the liver until we identified both the middle and right hepatic veins, and again it was possible to staple and divide these vessels. In a moment reminding me of some of the caesarean sections I had witnessed as a medical student, the resident and I gently wrestled the tumor mass out of the abdominal cavity, but, unlike the gentle swaddling of a newborn infant into a warm blanket, we indecorously plopped it into a very large basin we requested just for this purpose.
Returning our attention to the patient and the remaining portion of the left liver, we confirmed there was no bleeding or bile leak from the cut edge of the liver. Our blood loss for the operation was minimal. We checked the blood flow into and out of the liver using color flow ultrasonography. The liver was re-suspended to the diaphragm and the abdominal wall at the falciform ligament with a couple of sutures, and a drain was placed along the liver edge into the large empty space now present in the upper abdomen once occupied by a relatively gargantuan tumor. The patient recovered rapidly and without problems after her operation. She was young and in excellent health so she was walking the day after surgery and quickly developed a ravenous appetite. Nothing like having a large tumor compressing your stomach and intestine removed to improve your interest in food again. The patient was discharged from the hospital four days after the operation. Her drain tube was removed prior to discharge, and at her first post-operative visit she was recovering well and doing her best to ingest enough protein to permit liver regeneration. She succeeded well, and now has a large hypertrophied left lateral liver occupying her upper abdomen (see the representative image below).

On final pathology the patient did have a giant cavernous hemangioma, but the pathologist noted a few areas were worrisome for possible deterioration into a sarcoma-like situation. Her pathology slides were sent to multiple institutions and nobody was convinced she had an actual malignant tumor, but enough concern was raised I decided to follow her routinely for a few years to be certain no new tumors developed in the liver or at other sites. I saw her at six-month intervals with repeat MRI scans which confirmed there was no evidence of recurrent tumor. After about three years, I told her I was comfortable seeing her back on an annual basis. We did an annual visit and scans and blood tests were again completely normal. I had a social chat with the patient and her husband and learned she was involved in several new hobbies and activities. We ended the conversation with a pleasant goodbye and made plans for a visit a year later.
Seven months later I received an email from the patient requesting an urgent follow up appointment. Immediately alarmed and worried, I called my clinic staff to contact her for an appointment a few days later. When she arrived, I entered the examination room and was met by a somber-faced patient and her husband. She looked well but told me she was there to inform me of a new tumor. I asked if she was having symptoms to suggest the tumor had regrown. She solemnly shook her head no. I inquired if she had a disk with MRI scans for me to see. Another shake of the head no, and then she said, “All I have is this.” She handed me a black and white ultrasound image.
I’ve been a surgical oncologist for a long time, but thankfully my physical and mental facilities have not slowed yet. I studied the image for a few seconds, and by the time I looked up both my patient and her husband were grinning widely, and then openly laughing. She gleefully exclaimed, “I got you, didn’t I?”
Yes, yes you did. The ultrasound image revealed a normal human fetus of fourteen weeks gestation. I’ve performed thousands of ultrasounds of the liver, pancreas, and other upper abdominal organs or structures, but even though I’m not an obstetrician, I was quickly able to recognize the image of a human fetus. After the laughter and general hilarity waned and I congratulated them for playing the scene (and me) perfectly, we had an excited discussion about the elation and tribulations of parenthood. I shared stories from the time when my own children were small. I was thrilled for this young couple and this was not a conversation I had previously experienced in my practice. We agreed we would push the date of her next MRI scan to slightly longer than the originally planned one-year visit to allow her to complete her pregnancy.
A few weeks ago I noticed the patient’s name on my clinic schedule. I opened her MRI images and saw her enlarged left liver and no evidence of tumor recurrence. The scan also included the pelvic region and I noted a normal, non-pregnant uterus. I knocked once on the door, entered the room, and was immediately introduced to her new son. I have delivered lots of tumors out of patients’ bodies over the course of my career, but this remarkable, alert, healthy delivery brought a smile of pure happiness to my face. Removing malignant tumors from patients is rewarding, challenging, and often provides the best chance for a patient to be cured of this dread disease. I derive great satisfaction from the blessing of helping cancer patients, but holding this infant was a feeling of deep gratification surpassed only by the times years ago when I was embracing my own children. I hugged my patient and her husband and quickly reported everything was fine with her blood tests and scans. We spent the next twenty minutes watching her newborn son while talking about the fatigue, sleeplessness, and fulfillment associated with an infant. She was tired, but triumphant. As she left, she waved goodbye and stated, “I could have never had him with that huge tumor inside me.”
It certainly would have been crowded in her abdominal cavity with both a giant liver tumor and a full term infant present. I’m glad the removal of the liver tumor went so well and she is fully living and enjoying life. And more importantly, she has now created new life and will experience all of the joy, pleasure, fatigue, frustration, and induction of gray hair associated with this phenomenon.

We live in a remarkable time of advances in science and medicine. The human genome has been sequenced and mapped. Materials and drugs on a nanoscale are being designed and developed to treat cancer, infectious diseases, and other human medical … Continue reading

I have played sports throughout my life. Baseball, football, basketball, tennis, soccer, badminton, table tennis, running, cycling and even a short, and impressively painful, stint as a rugby winger. I would much rather play sports than watch sports. My wife … Continue reading
